I did a short (20 minute) talk at the Royal College of Psychiatrists International Conference recently, alongside Rob Poole (Chair), Linda Gask and Dariusz Galasinski. The title of the symposium was “The new anti-psychiatry” and Rob proposed it to the conference committee and it was accepted as three speakers and a chair, with significant time left for discussion.
We had an enjoyable and productive time both before and during the symposium, and the event was surprisingly well attended. As a bonus I also got to meet Samei Huda, which was a real treat.
Anyway, some rather special people who couldn’t be there suggested that I should do a version of the presentation as a blog, so here it is. I have included most of the slides from my talk here with a narrative that corresponds to what I said on the day in a slightly fuller way.
First, the title of the talk I gave was:
As a clinical psychologist, cognitive-behavioural therapist and mental health professional, I know a person’s perception of current events is shaped by the meaning they attach to such events, which in turn is influenced both by their values and previous “history”. “What happened to you?” is of course a key question which should always form part of our understanding of the way a person reacts to their present situation.
So; What happened to me and how might this relate to my reaction to the “Power Threat Meaning Framework” taking this as an example of current criticisms of psychiatry and clinical psychology. Hence the place of this presentation in the symposium.
Link to BPS publicity site for PTMFramework can be found here
How did my beliefs about psychiatry and anti-psychiatry form?
I qualified 40 years ago, Since then I have accumulated “lived experience” of the highs and lows of Psychiatry, mental health care and Clinical Psychology from the perspective of being a Clinical Psychologist and clinical researcher. I would also go as far as to say that, when I was in my first post-qualification job in Huddersfield (in lovely West Yorkshire, for those who don’t know!) this experience meant that I would have considered myself to be somewhat anti-psychiatry. This was a direct result of some obvious abuses of power and failures of care promulgated by some Consultant Psychiatrists I worked with. For example, I saw “maintenance ECT” being offered to large numbers of patients, I saw poly-pharmacy of epic proportions with horrific effects on service users. Insulin coma was being used and “abreaction” (“psychotherapy” under intravenous medication) was a frequent horror. Prolonged restraint and other abusive practices were common in the large long-stay hospital I spent time in, sometimes (but not always) pausing for as long as outsiders such as myself were in the building. So I was pretty “anti” all that appallingly bad practice.
It was also clear to me that poverty and discrimination were major determinants of psychological ill health which needed addressing but were largely ignored. My analysis of the situation at the time was that what I was seeing was some kind of assertion of medical supremacy and the valuing of “clinical experience” over evidence. Evidence was almost entirely disregarded except when it came in the form of Pharmaceutical company propaganda and incentives. I repeatedly argued with the consultant psychiatrists about a range of things including but not confined to benzodiazepine addiction, over-prescription in general and the need to move away from reliance on diagnosis onto formulation based approaches, something which came from (notably) Monte Shapiro, but which I had also learned from some very good psychiatry colleagues at the Maudsley. So, then as now, I was absolutely NOT anti-psychiatrist!
Forty years ago what were the clinical psychologists up to? Just like many of their psychiatrist colleagues, there was a tendency to reject evidence in favour of their “clinical experience”. There were a great many unqualified and frankly useless Psychologists. Even amongst those with an interest in evidence, some were embracing what we would now call “conversion therapy”; usually in the form of faradic aversion therapy (giving electric shocks to put people off being gay (Really!).
So yes, I was frequently anti psychiatry and sometimes anti clinical psychology BUT I also had the opportunity to connect with some wonderful, thoughtful and compassionate people who happened to be psychiatrists. We had great arguments and we were able to support and help a lot of people experiencing mental health problems.
Ok, so that was then. Is this still true for me?
Since then, Psychiatry has changed, and Clinical Psychology has changed. Clinical Psychology kept at its heart the importance of individual formulation, which in CBT developed into the idea of shared understanding and guided discovery. Diagnosis was there, and provided you weren’t stupid enough to believe that a diagnosis told you what a person’s problem was (but might help you consider where to look) then it was useful as an operationalisations of some key problems.
Fast forward some years and we have :
So the BPS/DCP express concern about diagnosis and call for a paradigm shift. Then we have a proposal called the Power Threat Meaning Framework, funded by the DCP, but not in any way approved by it or its membership. Matter of fact, the membership are given no say. Which is fine until the email announcing the setting up of the “implementation group” which reports directly to the DCP executive!


This all seemed very odd. I and others expressed concerns. The email is withdrawn….it was a mistake we are told.
Then about a year later, without explanation….
Who cares?
Ok, so why do I care if my professional organisation wants to implement this “new” framework?
Lets unpack my concern by first considering what the PTMF actually is. There is a fuller version of my summary and critique, co-written with an expert by experience (with whom I had no previous connection) here:
Power Threat Meaning Framework: innovative and important? #PTMFramework
In this, we sought to address the implication that the PTMF was “innovative and important”, concluding that what is innovative was not important, and what is important is not innovative.
Briefly here is the context
 .
.
So that’s a problem, reminiscent of other hard to understand texts, and strongly suggesting that its not intended for the public, but is rather focussed on a more academic/philosophical audience.
What does the PTMF really say?
I tried to summarise the core of PTMF in a Tweet, and this is what I ended up with
 In my view thats not too bad as a summary.
In my view thats not too bad as a summary.
Surely its all about the narrative?
So now to the narrative underpinning the framework, not least because the authors indicate that narrative is crucial, something I agree wholeheartedly with.
It all starts well; we have some statements which are about as close to truth as we get in psychology and psychiatry. BUT: these are mixed in with some blatant non-sequiturs. The problem, in my view, is the implication that to disagree with the non-sequiturs can be taken as disagreement with the other better supported statements. Things are much more nuanced than this. Adversity and Trauma can and do have serious effects but it does not follow that the application of the power-threat-meaning framework should therefore be used instead of best practice empirically grounded psychological or psychiatric approaches. To reject the PTMF package does not mean that you deny the importance of trauma in mental health, or that you are foolish enough to believe that psychiatric diagnosis tells you what a person’s problem actually is. There are some important points made, but they are not innovative.
There is much more that could be said about the “seven provisional patterns” proposed in the framework; I express my concerns about these in the Mental Elf blog if you are interested. Suffice it to say that I found it really astonishing to see this anti-diagnosis group propose seven diagnoses based on untenable claims about causation of mental health difficulties. This innovation is not important.
So, that brings me back to my early experience of bad psychiatry and crappy clinical psychology. What’s the connection? In my view it’s this:
Underpinning my “anti-psychiatry” back in the 1970s, and my concerns about clinical psychology at the same time was the reliance on clinical judgement and untestable theories. Yes, I quite like the ideas of Karl Popper. My view is that good clinical psychology (and Psychiatry) is a skilful blend of clinical art and clinical science. Such a blend is driven by empirical grounding, which includes but is not confined to both evidence based approaches and testable theories which evolve thorough quality research sensitive to threats to validity. To reject positivism is to take us back to the dark ages of our field, where clinicians followed their whims. Paul Meehl said something along the lines that people make the same mistake for 25 years and make a virtue of it by calling it their clinical experience. That was what I was seeing in both psychiatry and psychology forty years ago, and I don’t want to go back to those days. In my opinion, PTMF risks doing just that, and the signs so far are not reassuring.
Paradoxically, significant proportions of the early PTMFramework chapters seek to draw on some very positivist research in a highly selective way in an attempt to demonstrate social “causal” influences in MH. That’s a serious problem, because so far we have not been able to identify any “causal” factors in MH at all. Moderators, sure, but not causes. Those of us who are “positivists” have focussed on research which helps us to identify why some people experience problems which are particularly severe and particularly persistent. There is pretty decent evidence that dealing with these key maintaining factors is very helpful for those with MH problems, so we keep on trying to refine this work. Overall research in mental health focussed on the three key factors of Development, Delivery and Dissemination, and we are making headway in all of these domains. But causes? We know next to nothing. And of course, it probably goes without saying that the appropriate positioning is not anti-anything, but is pro-helping, blind to professional affiliation.
Why bother with positivism? Surely we and those who seek help from us just know when things work?
Lets take one of the key points made by PTMFramework for delivery of MH treatment; the importance of trauma focussed practice. Fundamentally I agree with this point (MH care should IMO deal with trauma where present as part of an integrated approach, collaboratively developed with the service user) but its JUST NOT ENOUGH to just say this. What kind of trauma focussed approach and how will it be applied? We know now that harms can be caused.
Mayou, Ehlers and Hobbs (2000) DOI: https://doi.org/10.1192/bjp.176.6.589
This remarkable paper changed the world in my view by demonstrating that a brief, well intentioned, credible and well delivered psychological intervention not only did not help but actually caused harm, which endured for at least three years. It made people worse.
I recall, back in my “anti-psychiatry” days, receiving a referral from one of the consultant psychiatrists with whom I regularly clashed. He said something along the lines of “We’ve tried hospital treatment, every drug we have in high doses and a bit of ECT so I don’t suppose that psychological therapy can do any harm”. What I didn’t say then but am saying now is that inappropriate psychologically informed approaches can and do harm, in a similar way as most likely was done by what preceded the referral. Just because its trauma informed does NOT mean that it is helpful, and indeed trauma informed care can turn out to be harmful, as the Mayou study demonstrates.
There has been another example recently brought to my attention. This one is particularly weird, and linked to PTMF appendix 7 (Trauma informed care pathways). There is a publication relevant to it:
Here’s the surprising if not shocking data from that document.
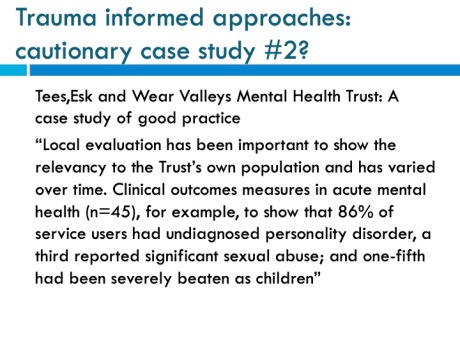
I find this literally incredible, but so far been unable to get clarification of it. I really really hope that this is not true. Let’s be clear regarding my potential bias in this respect. I consider personality disorder DIAGNOSIS to be horrifically bad practice, for lots of reasons including these studies:
https://onlinelibrary.wiley.com/doi/abs/10.1111/bjc.12093
If it is really true that the brand of trauma informed care use in Tees, Ask and Wear resulted in almost all those seen in acute psychiatry services getting PD diagnoses, then that should sound very loud alarm bells. “Trauma informed care” cannot simply be a mantra to be applied on the basis of ideology, but rather an approach to be evaluated in the context Quality Improvement Research and empirical grounding.
Rejection of positivism is the worst thing we can do. Think Baby-Bathwater
It seems to me that the PTMFramework suggests that MH should back away from empirically grounded and evidence based approaches. The reality is that, although MH care is a very long way from being good enough, it has over the last 40 years improved through a process of refinement stemming from a positivist approach. Yes, we can measure things and therefore find ways of doing things better (and stopping doing the useless things). To take any of the good elements identified in PTMF forward in my view this has to be from an empirically grounded positivist perspective. How else would we know if the framework as a whole (or elements of it) is helpful, pointless or even toxic to those we seek to help? The seven provisional patterns are clearly seven Alt-diagnoses; how might services users and MH professionals perceive these, and might their adoption be helpful for those to whom they are applied?
I have managed to be at odds with the DCP for a good portion of my career, and this doesn’t look like changing any time soon. The idea that a small group of psychologists with a couple of closely aligned EbE can produce a framework (which was not peer reviewed nor subject to any primary research) that would then be implemented nationally is patently absurd. So why have the DCP set up a PTMF implementation committee? The not unrelated DCP “Beyond Diagnosis” Committee appears to have foundered and failed. I would assert that clinical psychology is at its best splendid; in my view, that is when it takes the form of an applied science linked to understanding, caring and kindness. This is not the PTMF, which can and should be given the opportunity to prove itself not by DCP and BPS dictat but through proper discussion and scientific (including positivist) evaluation. It may or not be anti psychiatry, but it is most definitely not pro psychiatry or even pro working together, which in my view is profoundly sad. Why can’t we be critical friends, working together? I think we are good at that when we do it and when we seek to include service users as partners.
Conclusion
In conclusion, my experience tells me that anti-(bad-)psychiatry was justified precisely because, without saying so, many of those involved in it 40 years ago were IMPLICITLY anti-positivist in that they simply rejected empirical grounding in favour of their own inflated sense of wisdom. A similar approach characterised much of clinical psychology, with CPs bemoaning that they did not have the powerful positions that their psychiatric colleagues were abusing. Later bio-psychiatry suffered from a different malaise of complex and theory free speculation bolstered by poorly conceive and conducted studies in which the theoretical underpinnings were simply that the brain (or a neurotransmitter in it) was “faulty.” I commented elsewhere that the saddest aspect of the decade of the brain was that psychiatry lost its mind. Phenomenology was disregarded and dead fish showed brain activation in fMRI. This was not science, it was a colossal fishing expedition in more ways than one
Overall though there are reasons to be positive (but never complacent) about psychiatry and clinical psychology. There has definitely been evolution (but no paradigm shift or revolution) and increasing emphasis on more integrated theories and the beginnings of involvement of those with personal experience. However, when a group of clinical psychologists seek to implement an EXPLICITLY anti-positivist framework and seems to co-opt the Clinical Psychologists Professional body, the DCP, into this implementation, I am alarmed for the same reasons I found mainstream psychiatry to be damaging 40 years ago. I don’t care how we label it; here I’m offering it not only as an example of the new anti psychiatry, but also anti-clinical psychology. A plague on both your houses.
